OT SOAP Note Template (PDF & Word)
Streamline your documentation with this simple yet effective 3-page SOAP note template designed specifically for Occupational Therapists. Available in both PDF and editable Word formats, this tool offers flexibility for both digital and print use.
✨ Key Features in this Occupational Therapy SOAP Note Template:
Format Options:
• PDF – Write with a stylus directly or print for handwritten notes
• Word Doc – fully editable, with date pickers for convenience
Client & Session Details:
• Client name, therapist name, date of birth, session date & time
• Location (checkbox format)
Subjective Section:
• Client report, caregiver/family input, treatment goals
• Relevant medical history
Objective Section:
• Therapeutic activity & functional performance
• Client function checkboxes: Independent, Min/Mod/Max Assist, Dependent
• Assistive devices, environmental factors, and skills observed
Assessment Section:
• Progress toward goals & client response
• Rehab potential (checkbox + space for notes)
• Barriers to progress, clinical interpretation
Plan Section:
• Focus for next session, home program, referrals
• Intervention plan modifications
• Next session date/time & therapist signature
This OT SOAP Note template makes your documentation clear, compliant, and efficient—perfect for daily clinical use, student training, or private practice.
OT SOAP Note Template (PDF & Word)
Streamline your documentation with this simple yet effective 3-page SOAP note template designed specifically for Occupational Therapists. Available in both PDF and editable Word formats, this tool offers flexibility for both digital and print use.
✨ Key Features in this Occupational Therapy SOAP Note Template:
Format Options:
• PDF – Write with a stylus directly or print for handwritten notes
• Word Doc – fully editable, with date pickers for convenience
Client & Session Details:
• Client name, therapist name, date of birth, session date & time
• Location (checkbox format)
Subjective Section:
• Client report, caregiver/family input, treatment goals
• Relevant medical history
Objective Section:
• Therapeutic activity & functional performance
• Client function checkboxes: Independent, Min/Mod/Max Assist, Dependent
• Assistive devices, environmental factors, and skills observed
Assessment Section:
• Progress toward goals & client response
• Rehab potential (checkbox + space for notes)
• Barriers to progress, clinical interpretation
Plan Section:
• Focus for next session, home program, referrals
• Intervention plan modifications
• Next session date/time & therapist signature
This OT SOAP Note template makes your documentation clear, compliant, and efficient—perfect for daily clinical use, student training, or private practice.

 Image 1 of 7
Image 1 of 7
 Image 2 of 7
Image 2 of 7
 Image 3 of 7
Image 3 of 7
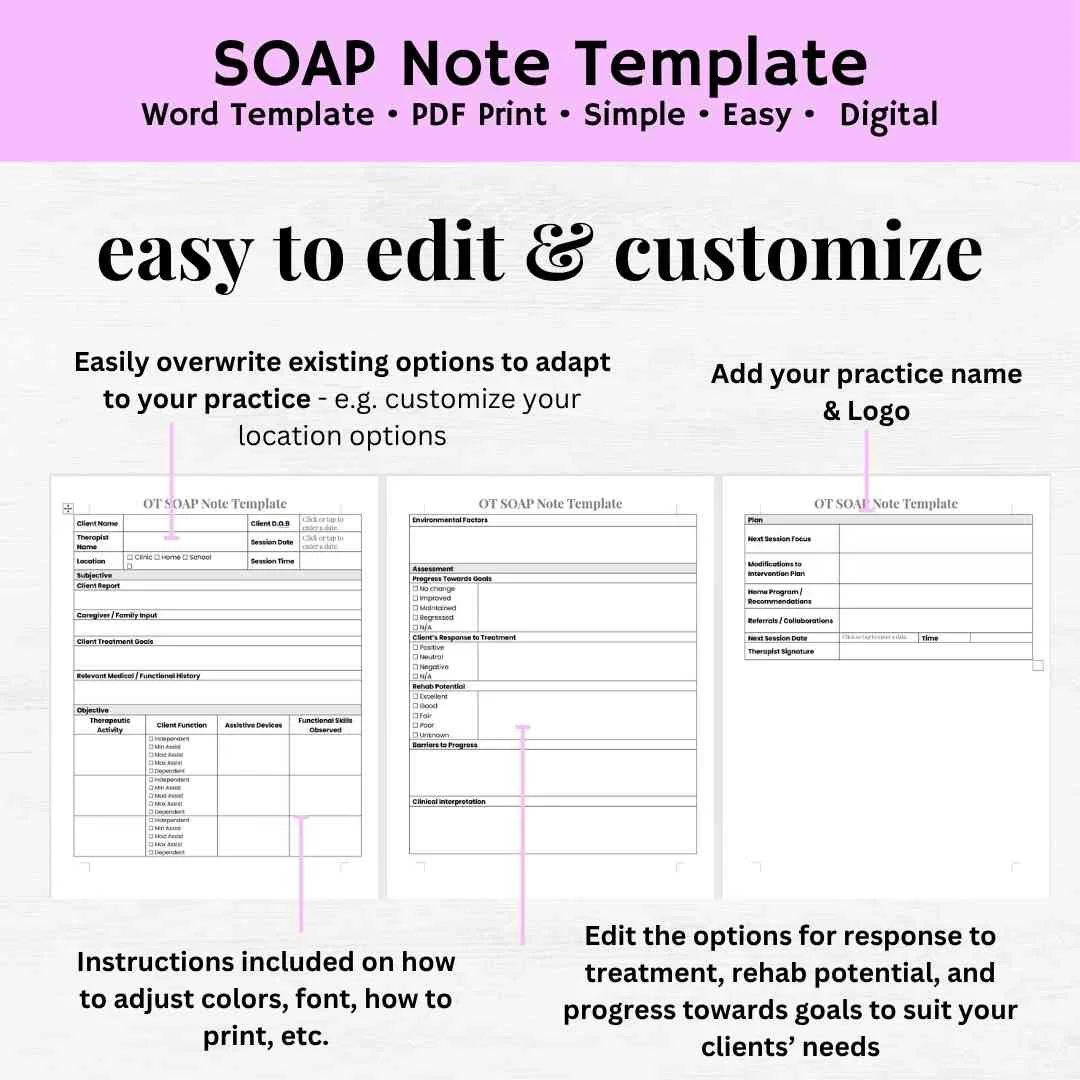 Image 4 of 7
Image 4 of 7
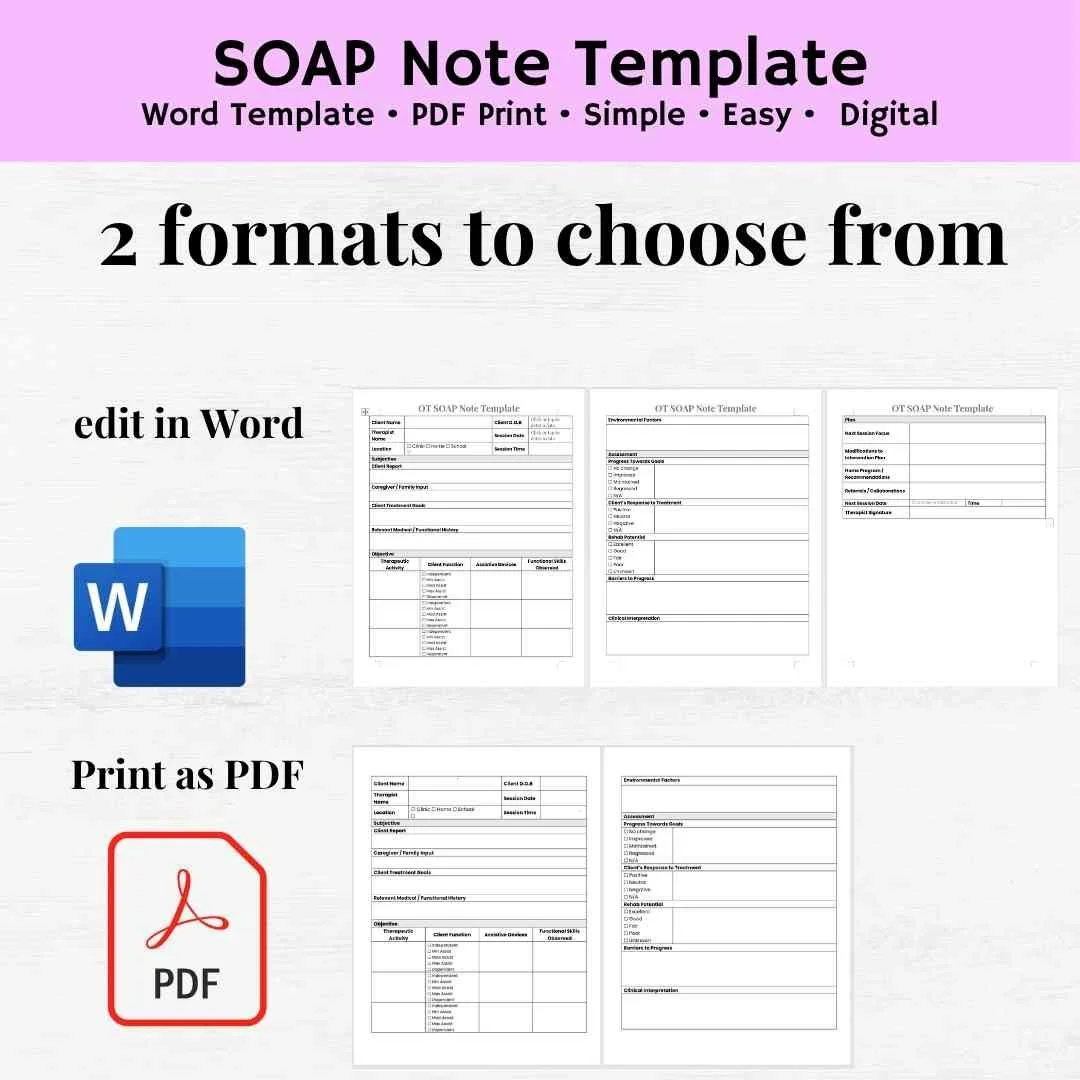 Image 5 of 7
Image 5 of 7
 Image 6 of 7
Image 6 of 7
 Image 7 of 7
Image 7 of 7